
| 产品编号 | bsm-51683M |
| 英文名称 | Lamin A/C Mouse mAb |
| 中文名称 | 核纤层蛋白A/C单克隆抗体 |
| 别 名 | lamin-A; CDCD1; CDDC; CMD1A; CMT2B1; EMD2; FPL; FPLD; FPLD2; HGPS; IDC; LDP1; LFP; LGMD1B; LMN1; LMNC; LMNL1; MADA; PRO1; Dhe; LMNA_CHICK; LMNA; LMNA_HUMAN; LMNA_MOUSE; LMNA_PIG; LMNA_RAT; |
| 研究领域 | 细胞生物 细胞凋亡 细胞类型标志物 Alzheimer's |
| 抗体来源 | Mouse |
| 克隆类型 | Monoclonal |
| 克 隆 号 | C3S4 |
| 交叉反应 | Human,Mouse,Rat |
| 产品应用 | WB=1:500-2000,IHC-P=1:100-500,IHC-F=1:100-500,IF=1:100-500
not yet tested in other applications. optimal dilutions/concentrations should be determined by the end user. |
| 理论分子量 | 73 kDa |
| 检测分子量 | 65-70 |
| 细胞定位 | 细胞核 |
| 性 状 | Liquid |
| 浓 度 | 1mg/ml |
| 免 疫 原 | Recombinant human Lamin A/C. |
| 亚 型 | IgG1, k |
| 纯化方法 | affinity purified by Protein G |
| 缓 冲 液 | 0.01M TBS (pH7.4) with 1% BSA, 0.02% Proclin300 and 50% Glycerol. |
| 保存条件 | Shipped at 4℃. Store at -20℃ for one year. Avoid repeated freeze/thaw cycles. |
| 注意事项 | This product as supplied is intended for research use only, not for use in human, therapeutic or diagnostic applications. |
| PubMed | PubMed |
| 产品介绍 |
Nuclear lamins form a network of intermediate-type filaments at the nucleoplasmic site of the nuclear membrane. Two main subtypes of nuclear lamins can be distinguished, i.e. A type lamins and B type lamins. The A type lamins comprise a set of three proteins arising from the same gene by alternative splicing, i.e. lamin A, lamin C and lamin Adel 10, while the B type lamins include two proteins arising from two distinct genes, i.e. lamin B1 and lamin B2. Recent evidence has revealed that mutations in A-type lamins give rise to a range of rare but dominant genetic disorders, including Emery-Dreifuss muscular dystrophy, dilated cardiomyopathy with conduction-system disease and Dunnigan-type familial partial lipodystrophy. In addition, the expression of A type lamins coincides with cell differentiation and as A type lamins specifically interact with chromatin, a role in the regulation of differential gene expression has been suggested for A type lamins. Function: Lamins are components of the nuclear lamina, a fibrous layer on the nucleoplasmic side of the inner nuclear membrane, which is thought to provide a framework for the nuclear envelope and may also interact with chromatin. Lamin A and C are present in equal amounts in the lamina of mammals. Play an important role in nuclear assembly, chromatin organization, nuclear membrane and telomere dynamics. Prelamin-A/C can accelerate smooth muscle cell senescence. It acts to disrupt mitosis and induce DNA damage in vascular smooth muscle cells (VSMCs), leading to mitotic failure, genomic instability, and premature senescence. Subunit: Homodimer of lamin A and lamin C. Interacts with lamin-associated polypeptides IA, IB and TMPO-alpha, RB1 and with emerin. Interacts with SREBF1, SREBF2, SUN2 and TMEM43. Proteolytically processed isoform A interacts with NARF. Interacts with SUN1. Prelamin-A/C interacts with EMD. Interacts with MLIP; may regulate MLIP localization to the nucleus envelope. Interacts with DMPK; may regulate nuclear envelope stability. Subcellular Location: Nucleus. Nucleus envelope. Note=Farnesylation of prelamin-A/C facilitates nuclear envelope targeting and subsequent cleaveage by ZMPSTE24/FACE1 to remove the farnesyl group produces mature lamin-A/C, which can then be inserted into the nuclear lamina. EMD is required for proper localization of non-farnesylated prelamin-A/C. Tissue Specificity: In the arteries, prelamin-A/C accumulation is not observed in young healthy vessels but is prevalent in medial vascular smooth muscle cells (VSMCs) from aged individuals and in atherosclerotic lesions, where it often colocalizes with senescent and degenerate VSMCs. Prelamin-A/C expression increases with age and disease. In normal aging, the accumulation of prelamin-A/C is caused in part by the down-regulation of ZMPSTE24/FACE1 in response to oxidative stress. Post-translational modifications: Increased phosphorylation of the lamins occurs before envelope disintegration and probably plays a role in regulating lamin associations. Proteolytic cleavage of the C-terminal of 18 residues of prelamin-A/C results in the production of lamin-A/C. The prelamin-A/C maturation pathway includes farnesylation of CAAX motif, ZMPSTE24/FACE1 mediated cleavage of the last three amino acids, methylation of the C-terminal cysteine and endoproteolytic removal of the last 15 C-terminal amino acids. Proteolytic cleavage requires prior farnesylation and methylation, and absence of these blocks cleavage. Sumoylation is necessary for the localization to the nuclear envelope. Farnesylation of prelamin-A/C facilitates nuclear envelope targeting. DISEASE: Defects in LMNA are the cause of Emery-Dreifuss muscular dystrophy type 2, autosomal dominant (EDMD2) [MIM:181350]. A degenerative myopathy characterized by weakness and atrophy of muscle without involvement of the nervous system, early contractures of the elbows, Achilles tendons and spine, and cardiomyopathy associated with cardiac conduction defects. Defects in LMNA are the cause of Emery-Dreifuss muscular dystrophy type 3, autosomal recessive (EDMD3) [MIM:181350]. Defects in LMNA are the cause of cardiomyopathy dilated type 1A (CMD1A) [MIM:115200]. Dilated cardiomyopathy is a disorder characterized by ventricular dilation and impaired systolic function, resulting in congestive heart failure and arrhythmia. Patients are at risk of premature death. Defects in LMNA are the cause of familial partial lipodystrophy type 2 (FPLD2) [MIM:151660]; also known as familial partial lipodystrophy Dunnigan type. A disorder characterized by the loss of subcutaneous adipose tissue in the lower parts of the body (limbs, buttocks, trunk). It is accompanied by an accumulation of adipose tissue in the face and neck causing a double chin, fat neck, or cushingoid appearance. Adipose tissue may also accumulate in the axillae, back, labia majora, and intraabdominal region. Affected patients are insulin-resistant and may develop glucose intolerance and diabetes mellitus after age 20 years, hypertriglyceridemia, and low levels of high density lipoprotein cholesterol. Defects in LMNA are the cause of limb-girdle muscular dystrophy type 1B (LGMD1B) [MIM:159001]. LGMD1B is an autosomal dominant degenerative myopathy with age-related atrioventricular cardiac conduction disturbances, dilated cardiomyopathy, and the absence of early contractures. LGMD1B is characterized by slowly progressive skeletal muscle weakness of the hip and shoulder girdles. Muscle biopsy shows mild dystrophic changes. Defects in LMNA are the cause of Charcot-Marie-Tooth disease type 2B1 (CMT2B1) [MIM:605588]. CMT2B1 is a form of Charcot-Marie-Tooth disease, the most common inherited disorder of the peripheral nervous system. Charcot-Marie-Tooth disease is classified in two main groups on the basis of electrophysiologic properties and histopathology: primary peripheral demyelinating neuropathy or CMT1, and primary peripheral axonal neuropathy or CMT2. Neuropathies of the CMT2 group are characterized by signs of axonal regeneration in the absence of obvious myelin alterations, normal or slightly reduced nerve conduction velocities, and progressive distal muscle weakness and atrophy. CMT2B1 inheritance is autosomal recessive. Defects in LMNA are the cause of Hutchinson-Gilford progeria syndrome (HGPS) [MIM:176670]. HGPS is a rare genetic disorder characterized by features reminiscent of marked premature aging. Note=HGPS is caused by the toxic accumulation of a mutant form of lamin-A/C. This mutant protein, called progerin, acts to deregulate mitosis and DNA damage signaling, leading to premature cell death and senescence. Progerin lacks the conserved ZMPSTE24/FACE1 cleavage site and therefore remains permanently farnesylated. Thus, although it can enter the nucleus and associate with the nuclear envelope, it cannot incorporate normally into the nuclear lamina. Defects in LMNA are the cause of cardiomyopathy dilated with hypergonadotropic hypogonadism (CMDHH) [MIM:212112]. A disorder characterized by the association of genital anomalies, hypergonadotropic hypogonadism and dilated cardiomyopathy. Patients can present other variable clinical manifestations including mental retardation, skeletal anomalies, scleroderma-like skin, graying and thinning of hair, osteoporosis. Dilated cardiomyopathy is characterized by ventricular dilation and impaired systolic function, resulting in congestive heart failure and arrhythmia. Defects in LMNA are the cause of mandibuloacral dysplasia with type A lipodystrophy (MADA) [MIM:248370]. A disorder characterized by mandibular and clavicular hypoplasia, acroosteolysis, delayed closure of the cranial suture, progeroide appearance, partial alopecia, soft tissue calcinosis, joint contractures, and partial lipodystrophy with loss of subcutaneous fat from the extremities. Adipose tissue in the face, neck and trunk is normal or increased. Defects in LMNA are a cause of lethal tight skin contracture syndrome (LTSCS) [MIM:275210]; also known as restrictive dermopathy (RD). Lethal tight skin contracture syndrome is a rare disorder mainly characterized by intrauterine growth retardation, tight and rigid skin with erosions, prominent superficial vasculature and epidermal hyperkeratosis, facial features (small mouth, small pinched nose and micrognathia), sparse/absent eyelashes and eyebrows, mineralization defects of the skull, thin dysplastic clavicles, pulmonary hypoplasia, multiple joint contractures and an early neonatal lethal course. Liveborn children usually die within the first week of life. The overall prevalence of consanguineous cases suggested an autosomal recessive inheritance. Defects in LMNA are the cause of heart-hand syndrome Slovenian type (HHS-Slovenian) [MIM:610140]. Heart-hand syndrome (HHS) is a clinically and genetically heterogeneous disorder characterized by the co-occurrence of a congenital cardiac disease and limb malformations. Defects in LMNA are the cause of muscular dystrophy congenital LMNA-related (MDCL) [MIM:613205]. It is a form of congenital muscular dystrophy. Patients present at birth, or within the first few months of life, with hypotonia, muscle weakness and often with joint contractures. Similarity: Belongs to the intermediate filament family. SWISS: P02545 Gene ID: 4000 Database links: Entrez Gene: 4000 Human Entrez Gene: 16905 Mouse SwissProt: P02545 Human SwissProt: P48678 Mouse |
| 产品图片 |
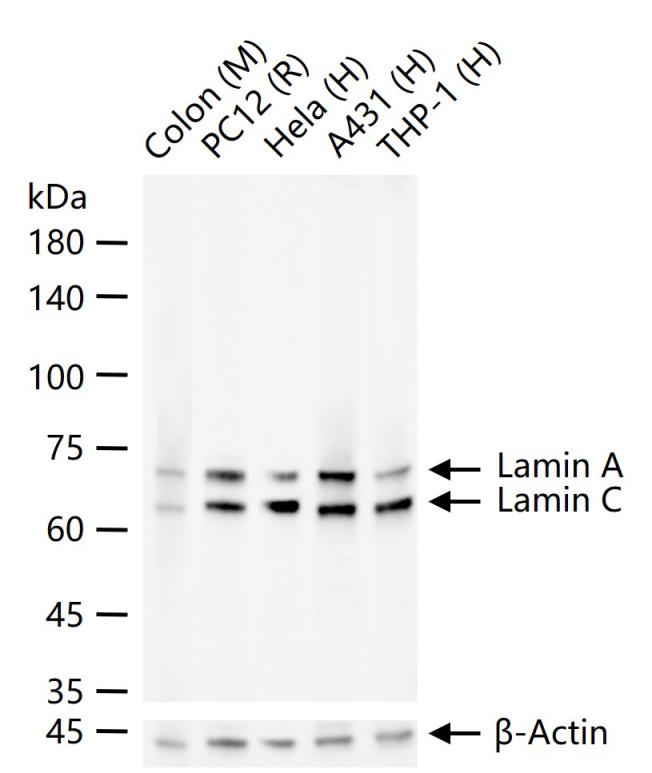
25 ug total protein per lane of various lysates (see on figure) probed with Lamin A/C monoclonal antibody, unconjugated (bsm-51683M) at 1:500 dilution and 4°C overnight incubation. Followed by conjugated secondary antibody incubation at r.t. for 60 min.
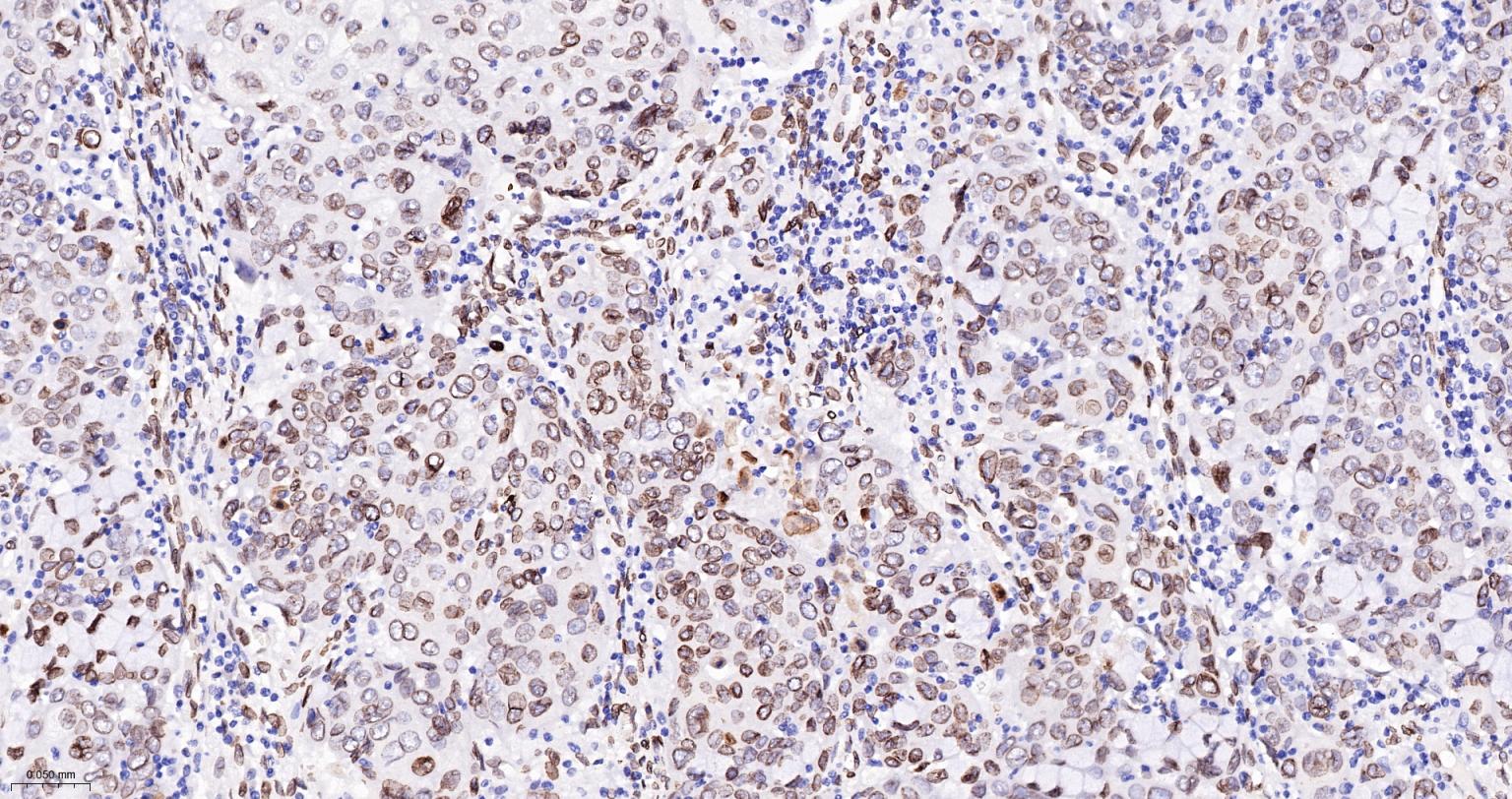
Paraformaldehyde-fixed, paraffin embedded Human Cervical Cancer; Antigen retrieval by boiling in sodium citrate buffer (pH6.0) for 15 min; The section was incubated with Lamin A/C Monoclonal Antibody, Unconjugated (bsm-51683M) at 1:100 overnight at 4°C, followed by conjugation to the bs-40296G-HRP and DAB (C-0010) staining.
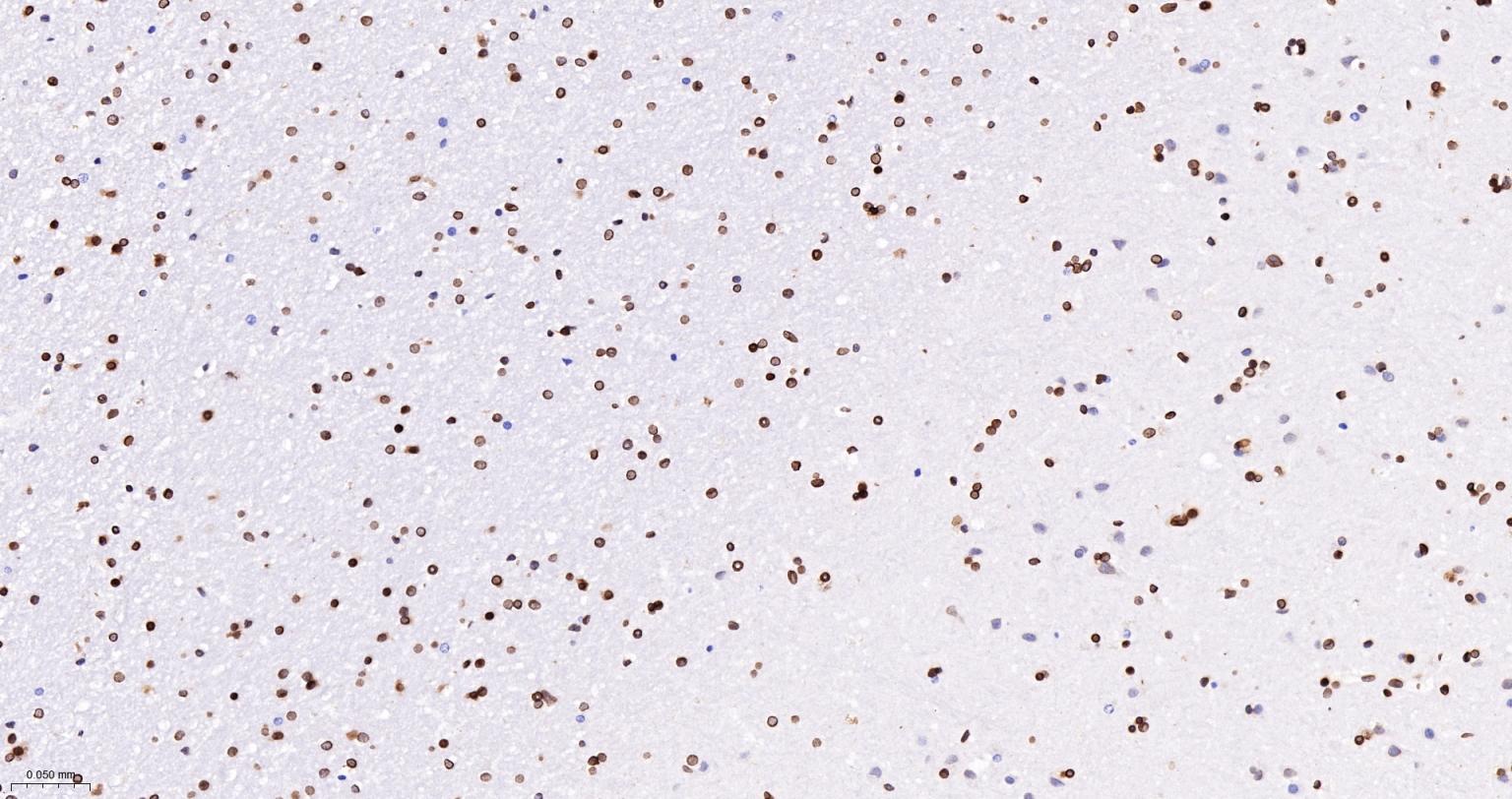
Paraformaldehyde-fixed, paraffin embedded Human Cerebrum; Antigen retrieval by boiling in sodium citrate buffer (pH6.0) for 15 min; The section was incubated with Lamin A/C Monoclonal Antibody, Unconjugated (bsm-51683M) at 1:100 overnight at 4°C, followed by conjugation to the bs-40296G-HRP and DAB (C-0010) staining.
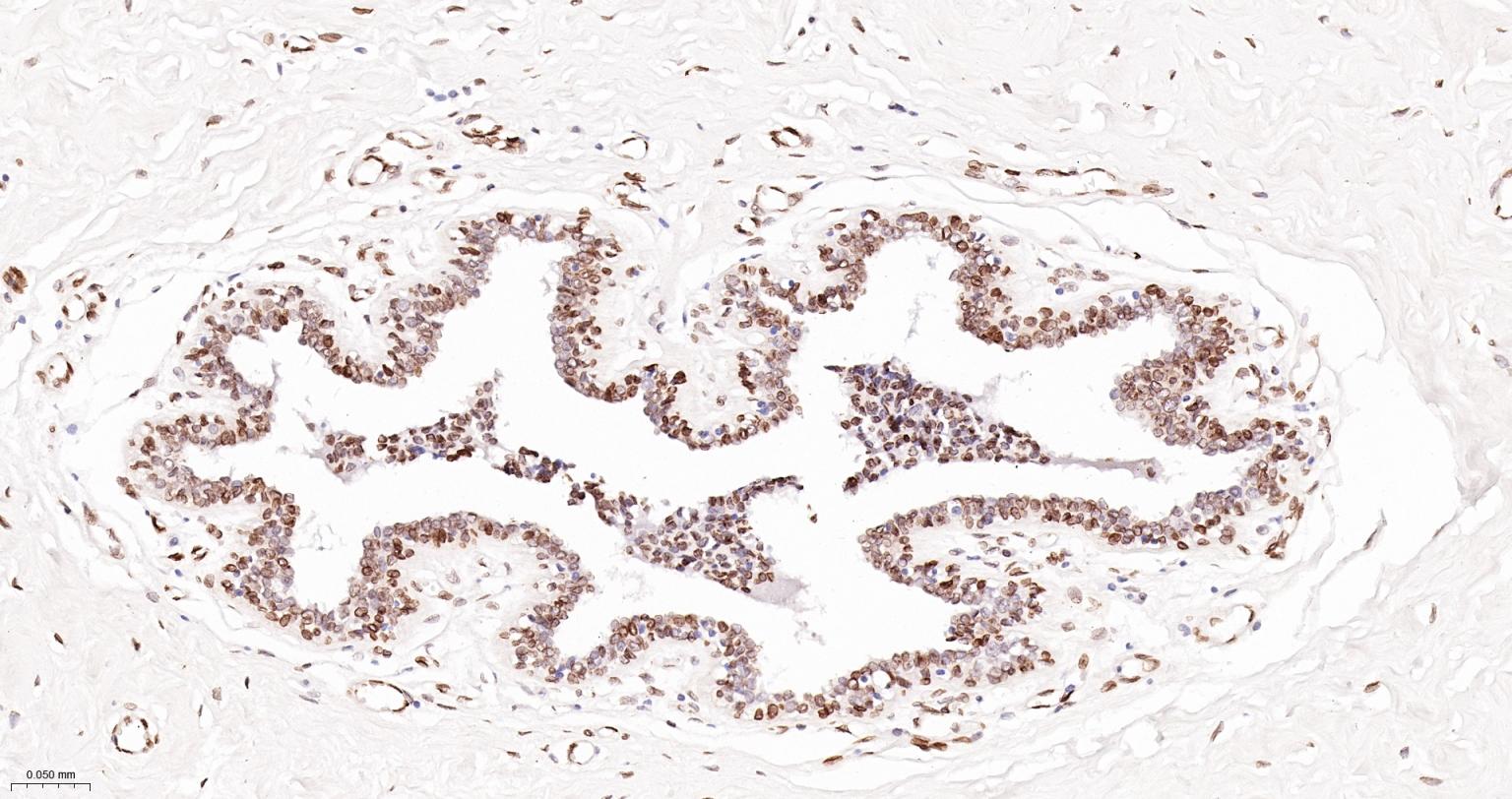
Paraformaldehyde-fixed, paraffin embedded Human Breast; Antigen retrieval by boiling in sodium citrate buffer (pH6.0) for 15 min; The section was incubated with Lamin A/C Monoclonal Antibody, Unconjugated (bsm-51683M) at 1:100 overnight at 4°C, followed by conjugation to the bs-40296G-HRP and DAB (C-0010) staining.
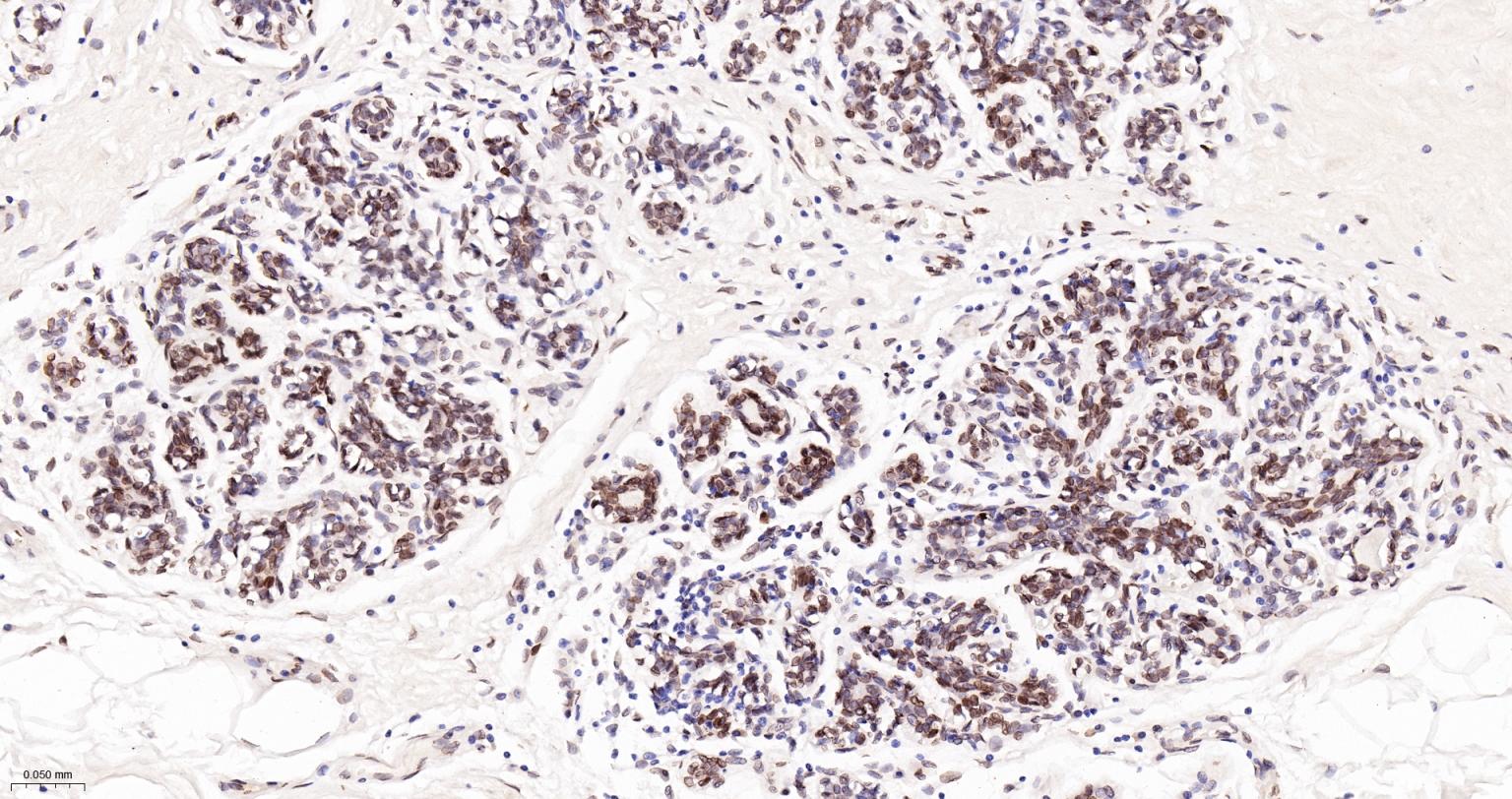
Paraformaldehyde-fixed, paraffin embedded Human Breast Cancer; Antigen retrieval by boiling in sodium citrate buffer (pH6.0) for 15 min; The section was incubated with Lamin A/C Monoclonal Antibody, Unconjugated (bsm-51683M) at 1:100 overnight at 4°C, followed by conjugation to the bs-40296G-HRP and DAB (C-0010) staining.
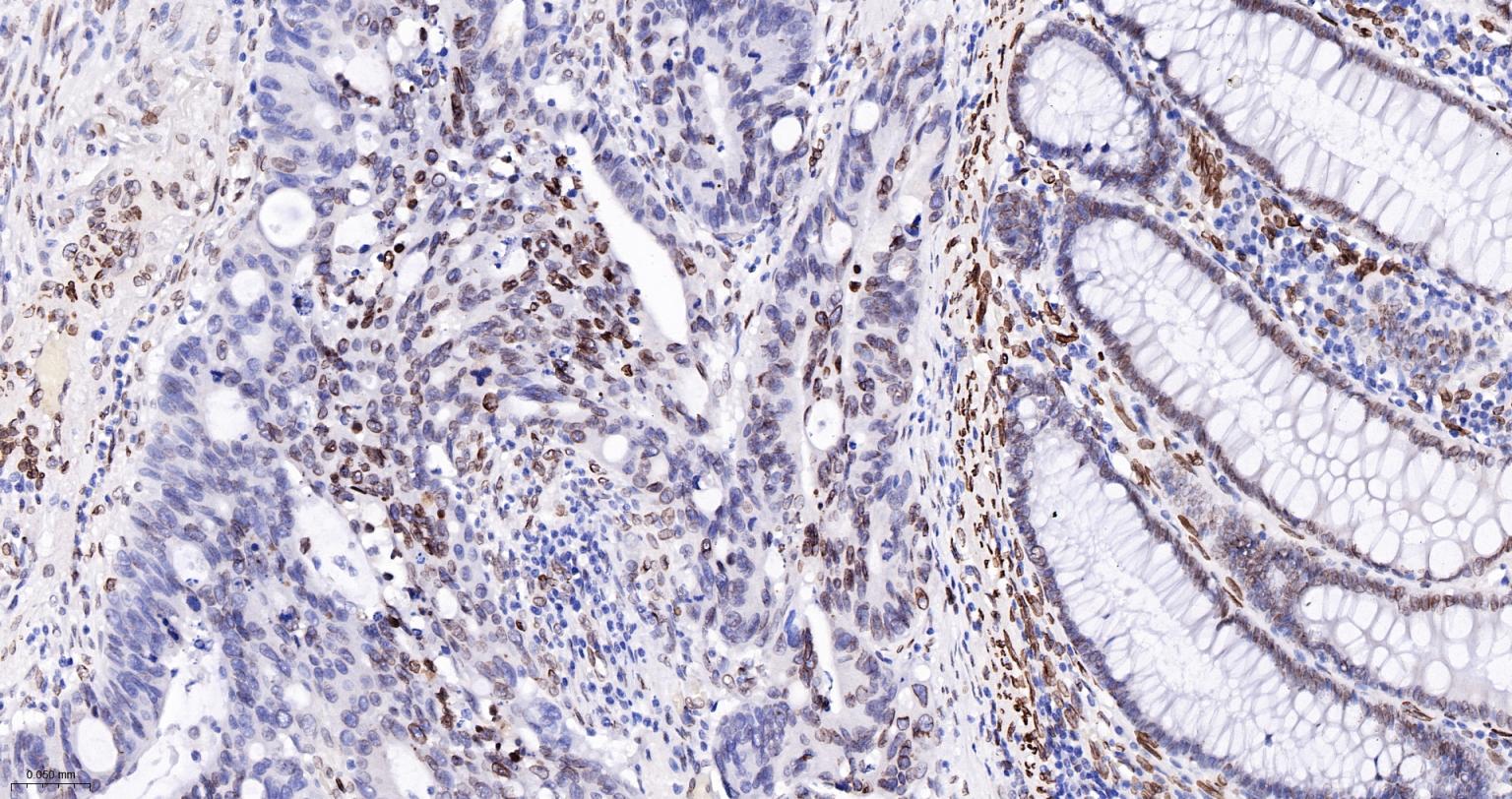
Paraformaldehyde-fixed, paraffin embedded Human Colon Cancer; Antigen retrieval by boiling in sodium citrate buffer (pH6.0) for 15 min; The section was incubated with Lamin A/C Monoclonal Antibody, Unconjugated (bsm-51683M) at 1:100 overnight at 4°C, followed by conjugation to the bs-40296G-HRP and DAB (C-0010) staining.
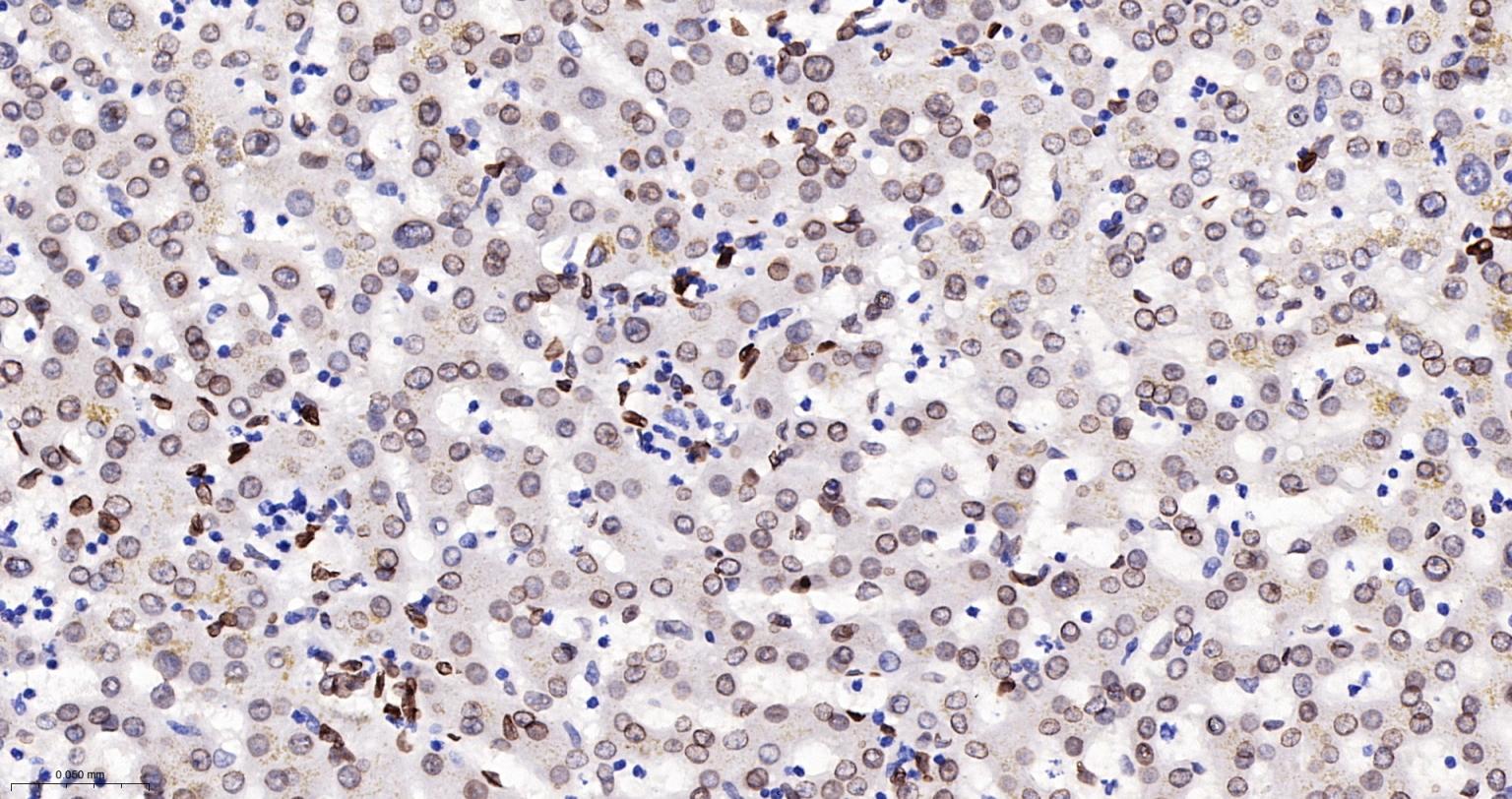
Paraformaldehyde-fixed, paraffin embedded Human Liver; Antigen retrieval by boiling in sodium citrate buffer (pH6.0) for 15 min; The section was incubated with Lamin A/C Monoclonal Antibody, Unconjugated (bsm-51683M) at 1:100 overnight at 4°C, followed by conjugation to the bs-40296G-HRP and DAB (C-0010) staining.
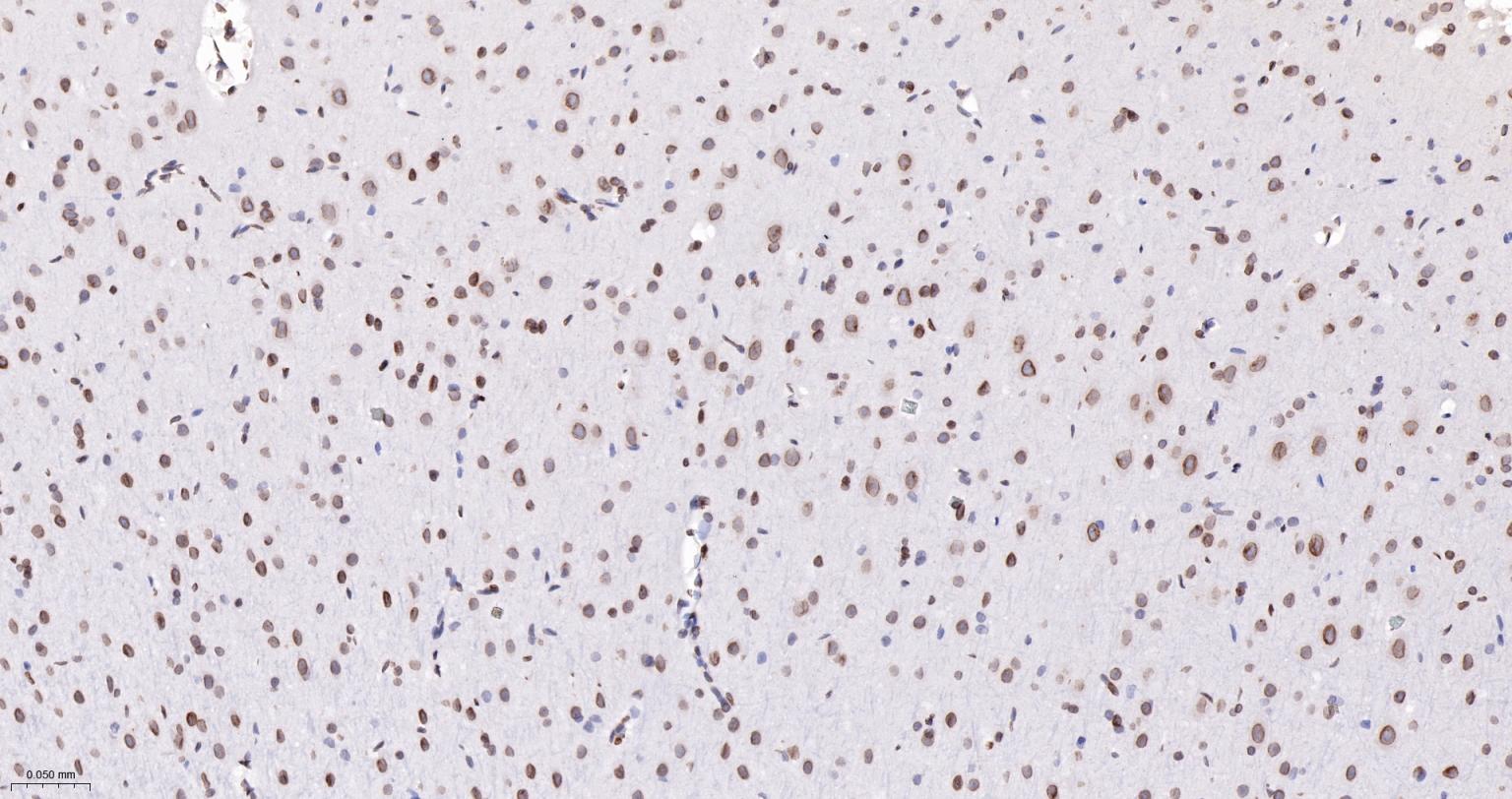
Paraformaldehyde-fixed, paraffin embedded Rat Cerebrum; Antigen retrieval by boiling in sodium citrate buffer (pH6.0) for 15 min; The section was incubated with Lamin A/C Monoclonal Antibody, Unconjugated (bsm-51683M) at 1:100 overnight at 4°C, followed by conjugation to the bs-40296G-HRP and DAB (C-0010) staining.
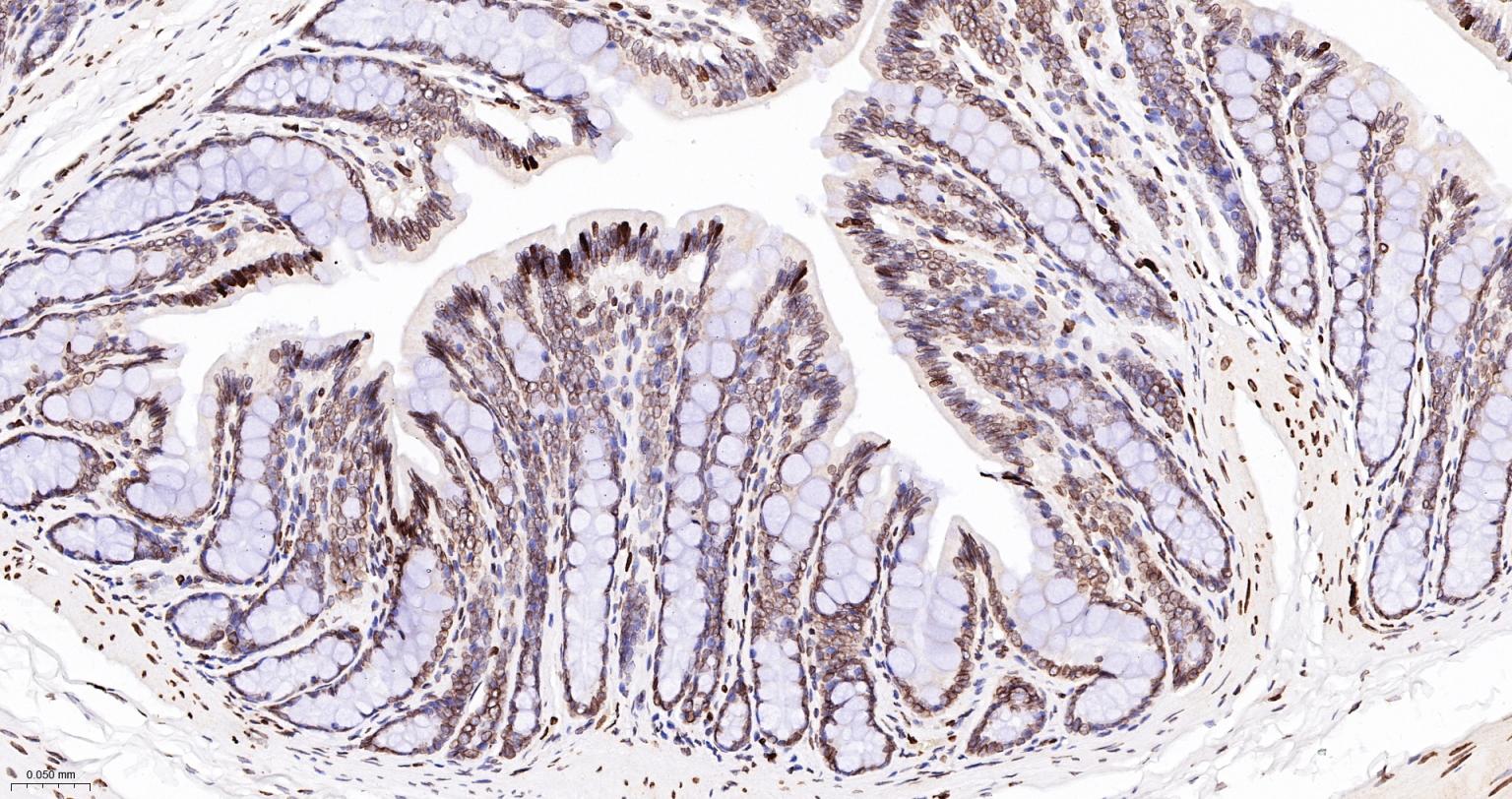
Paraformaldehyde-fixed, paraffin embedded Rat Colon; Antigen retrieval by boiling in sodium citrate buffer (pH6.0) for 15 min; The section was incubated with Lamin A/C Monoclonal Antibody, Unconjugated (bsm-51683M) at 1:100 overnight at 4°C, followed by conjugation to the bs-40296G-HRP and DAB (C-0010) staining.
|
| 1、抗体溶解方法 | |
| 2、抗体修复方式 | |
| 3、常用试剂的配制 | |
| 4、免疫组化操作步骤 | |
| 5、免疫组化问题解答 | |
| 6、Western Blotting 操作步骤 | |
| 7、Western Blotting 问题解答 | |
| 8、关于肽链的设计 | |
| 9、多肽的溶解与保存 | |
| 10、酶标抗体效价测定程序 | |




